Keep UPMC Pinnacle Lancaster Open: Write a Letter to the Editor by March 1st
Lancaster HRC is asking for solidarity from across the state in the struggle to keep UPMC Pinnacle Lancaster open and accountable to the people. Will you write a Letter to the Editor (LTE) to show where you stand?
Here’s a sample letter:
I’m from the ___________ Healthcare Rights Committee with Put People First! PA and I stand in solidarity with the Lancaster Healthcare Rights Committee against the closure of UPMC Pinnacle Lancaster.
It’s devastating to hear that UPMC Pinnacle has decided to close a much needed hospital in the Lancaster community. Hands Off! UPMC”
250 words or less – that simple. LTEs can be submitted directly to LNP in Lancaster or to your local news area. Please contact Jamie at Jamiebokanblair@gmail.com on the Media & Communications team if you have any questions or are interested in taking next steps.
Submit your Letter to the Editor before March 1st when the Hospital is slated to close. Here’s the round up of recent LTE’s — linked here with text below.
- Josh, Lancaster HRC member
- Lillyanna Brooks, Lancaster HRC member
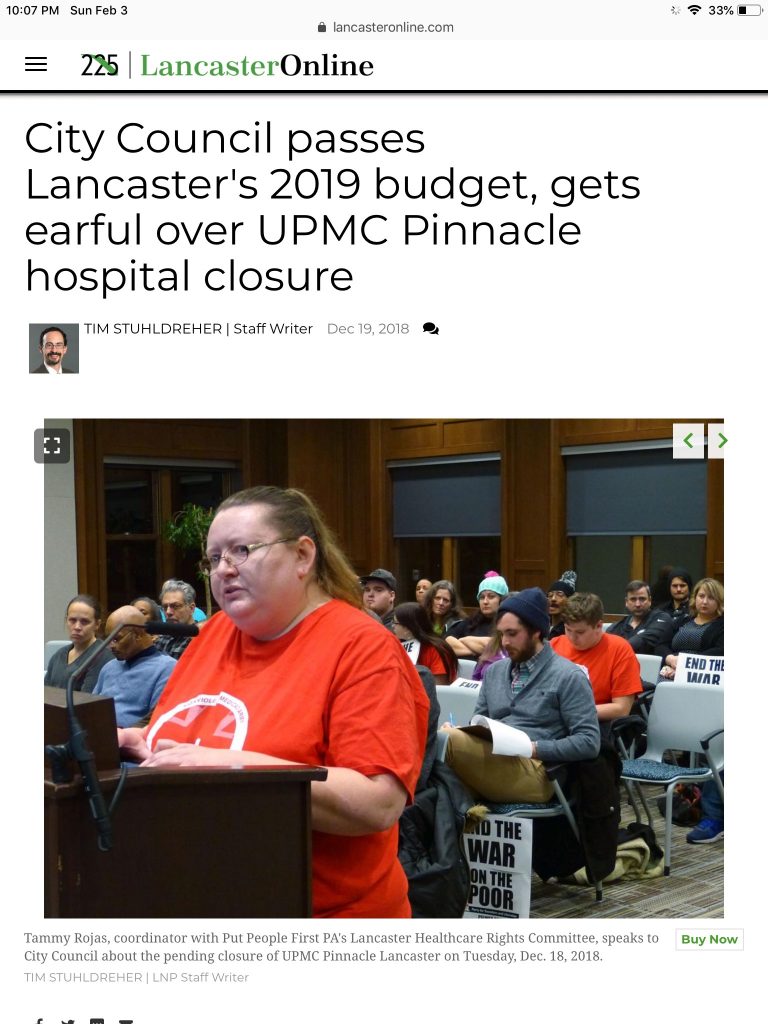
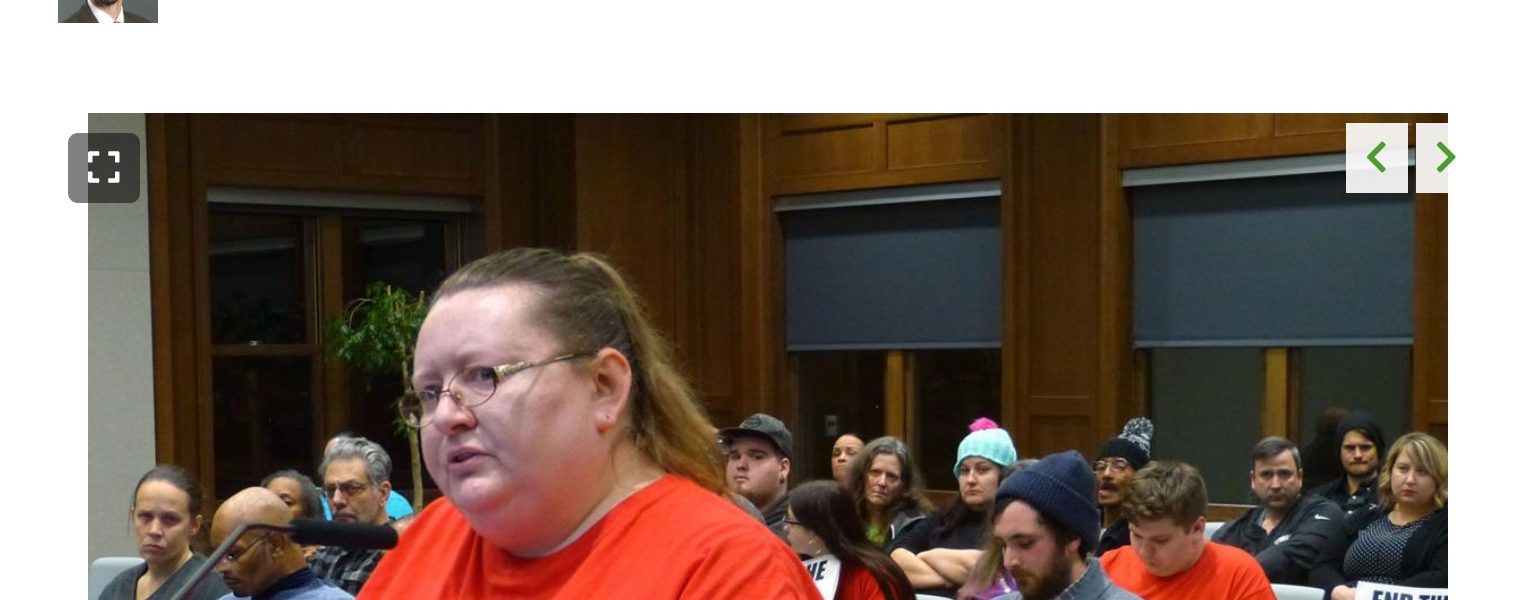
- Tammy, Lancaster HRC member
- Karim, Philly member
- Larry, Johnstown HRC member
- Barbara, Pittsburgh member
Josh, Lancaster — I am disgusted about the closing of the old Lancaster Regional Medical Center by UPMC Pinnacle. I believe it’s deadly, catastrophic and immoral.
We are potentially going to lose lives because of this closing, and all we can hear is “Our hands are tied.” This letter will not save the hospital, but it will make a good point and that point is directed at UPMC Pinnacle and our own politicians.
Whose side are you on? The people’s or UPMC Pinnacle? I know what side I am on, and I can’t wait to hear whose side you’re on.
Lillyanna Brooks, Lancaster — What do you get from shutting down UPMC Pinnacle Lancaster? Is it for bigger prodicts? Is it because you’re inhumane? There will be one hospital in Lancaster city. Many people will be losing their jobs. People might die because they will have to be transported about 30 minutes away to Lititz. Lancaster General Hospital will be overpacked.
UPMC Pinnacle Lancaster’s closing might cause Lancaster’s poverty rate to rise. Do we, the people of Lancaster, want this? If you don’t, stand up with us and fight UPMC. (Putpeoplefirstpa.org)
Tammy, Lancaster — I have seen the outcry from the community about the upcoming closing of UPMC Pinnacle Lancaster. I’m here to tell you: Don’t give up. We can unite as a community and solve this problem together. We at the Lancaster Healthcare Rights COmmittee, Put People First! PA, are currently working on the issue alongside other individuals in the community. We started by addressing Lancaster City Council during the last meeting of 2018 and are already working on the next steps.
We the people hold the power to make real and fundamental change happen in our communities as long as we unite to do so. We have the right to speak up and have our voices heard. We have a right to say what health care should look like in Lancaster. That’s why I joined {Put People First! PA and the Poor People’s Campaign: a National Call for Moral Revival, because I believe in the real power — the power of the people.
If we unite and take action together on this issue, forming bonds for future events, we will be a new and unsettling force in Lancaster. Join us at putpeoplefirstpa.org
Karim, Philadelphia — As a medical student getting ready to start residency, I’m dismayed by the closure of UPMC Pinnacle in Lancaster. Lancaster residents see Pinnacle, formerly St. Joseph’s Hospital, as a major pillar in their community, but it seems their needs and concerns weren’t a remote consideration here. It’s well known that primary care and social services are the main driver of health outcomes, but UPMC’s investments seem to be moving towards expensive specialty care for the already-sick in a wealthy city saturated with hospitals. They recently unveiled plans for a new cancer center, heart and transplant center, and a rehab center in Pittsburgh. From rotating at hospitals in Pittsburgh, Philadelphia, Danville, and Scranton, I’ve also seen the way big hospital systems engage in turf wars. Even medical students get involved in this. Our tuition dollars are assets to be exchanged between hospital and university systems, and we get shifted about accordingly. In Philadelphia, Jefferson is working to acquire the prestigious Fox Chase Cancer Center from Temple Health. The Temple University Board of Trustees had a transparent quote in a recent Philly Magazine article: “Currently, Temple Health again faces significant financial challenges. These challenges are primarily due to the fact that Temple Hospital is proportionally the largest provider of healthcare to Medicaid patients.” Are similar dynamics at play in the UPMC Pinnacle closure? We need transparency from UPMC, and there needs to be accountability for the downstream effects of divestment on health outcomes. It has implications for the whole state. Health care is a human right, not a commodity.
Larry, Johnstown — In regard to the proposed closing of UPMC Pinnacle Lancaster, I and many other members of Put People First! PA in Johnstown and statewide wish to express our support for the Lancaster Healthcare Rights Committee in its opposition to placing the profit-focused business decisions of UPMC over the health care needs of Lancaster residents.
Profit-focused hospitals are intensifying their efforts to dominate local and regional health care markets to enhance their bottom line (by reducing competition) at the expense of community health care needs.
At Put People First! PA, we believe people — whether in Johnstown, Lancaster or around the state and nation — are not markets, we are not profit centers or business opportunities. We are not commodities as part of some merger or acquisition, nor are we a part of someone’s investment portfolio. We are human beings, and we all need and demand the dignity of health care as a human right.
Join the Lancaster Healthcare Rights Committee and take a stand against UPMC Pinnacle Lancaster’s closing.
Barbara, Pittsburgh — I was disgusted to hear about UPMC closing UPMC Pinnacle Lancaster hospital without community input. This action by UPMC was hostile and immoral, and I’m glad members of the community are fighting it.
I immediately thought about UPMC Braddock hospital in Braddock, a poor and predominantly black Pittsburgh-area neighborhood, which UPMC closed Jan. 31, 2010, despite protests from residents.
Why should we allow UPMC to get away with building specialty hospitals in Pittsburgh and Sicily, Italy, while closing hospitals in poor communities? Everybody has a right to live and get the care we need!
I’m with the Pittsburgh Healthcare Rights Committee of Put People First! PA, and I stand in solidarity with the Lancaster Healthcare Rights Committee against the closure of UPMC Pinnacle Lancaster.
If UPMC doesn’t want to run the hospital, the city should take it and find another health care resource to take it over. It is a community asset and should not be destroyed or sacrificed to UPMC’s desire for profit.