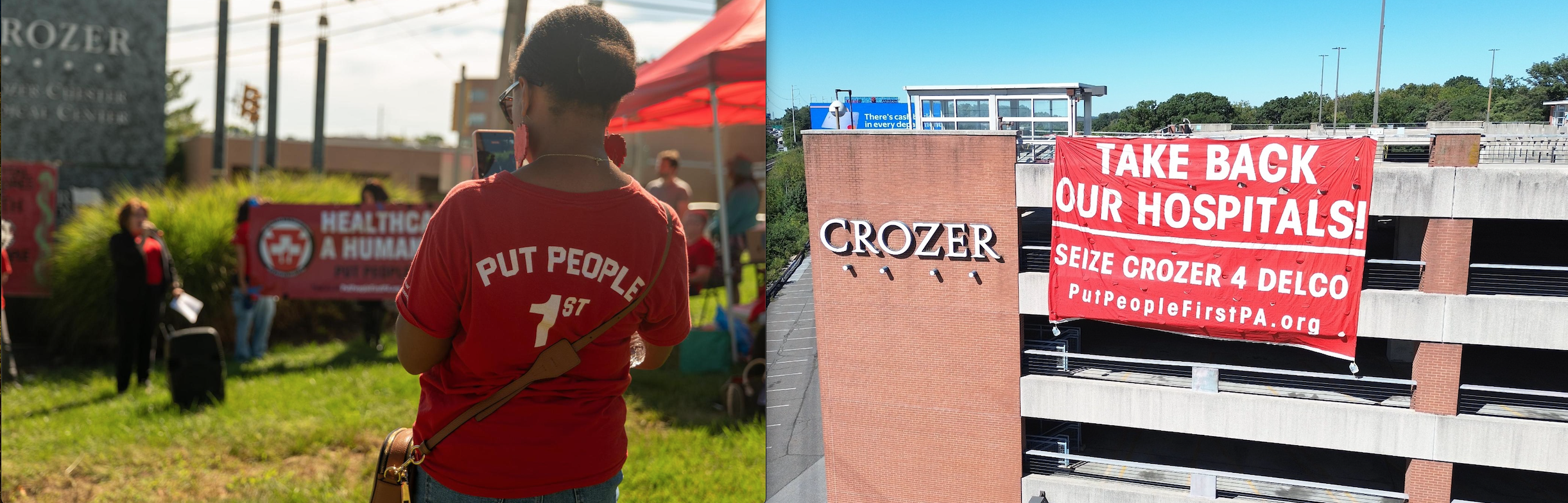
On May 2nd, Put People First! PA members from Southeast PA joined Chester Residents Concerned for Quality Living (CRCQL) and other local groups for a powerful action in Chester, Delaware County. The day began with a rally in front of Chester City Hall and continued with a 90 minute walk to the Reworld incinerator, formerly Covanta, which operates the largest trash incinerator in the country. The facility burns up to 3,500 tons of trash each day, releasing toxic air pollution linked to asthma, cancer, heart disease, and other serious illnesses.
Environmental justice is a healthcare issue. On the one‑year anniversary of the Crozer Chester Hospital closure, the action highlighted how one of the state’s poorest communities has been denied emergency care even as ruling‑class industrial pollution continues to endanger residents’ health.
Our participation strengthened our landscape assessment of Chester and the communities surrounding the hospital, while also deepening relationships with partner organizations. Along the march route, residents stepped out of their homes to wave and cheer, and a coordinated door‑knocking effort unfolded in tandem with the procession. Chants like “Let Chester Breathe” and “We Breathe All Day, We Breathe All Night, Clean Air Is a Human Right” highlighted the intersections between our campaigns. After the event, our team of eight gathered to debrief on what we had learned about our class and how our theory of change informs our organizing.
– Reportback by Southeast PA Healthcare Rights Committee member, Heather
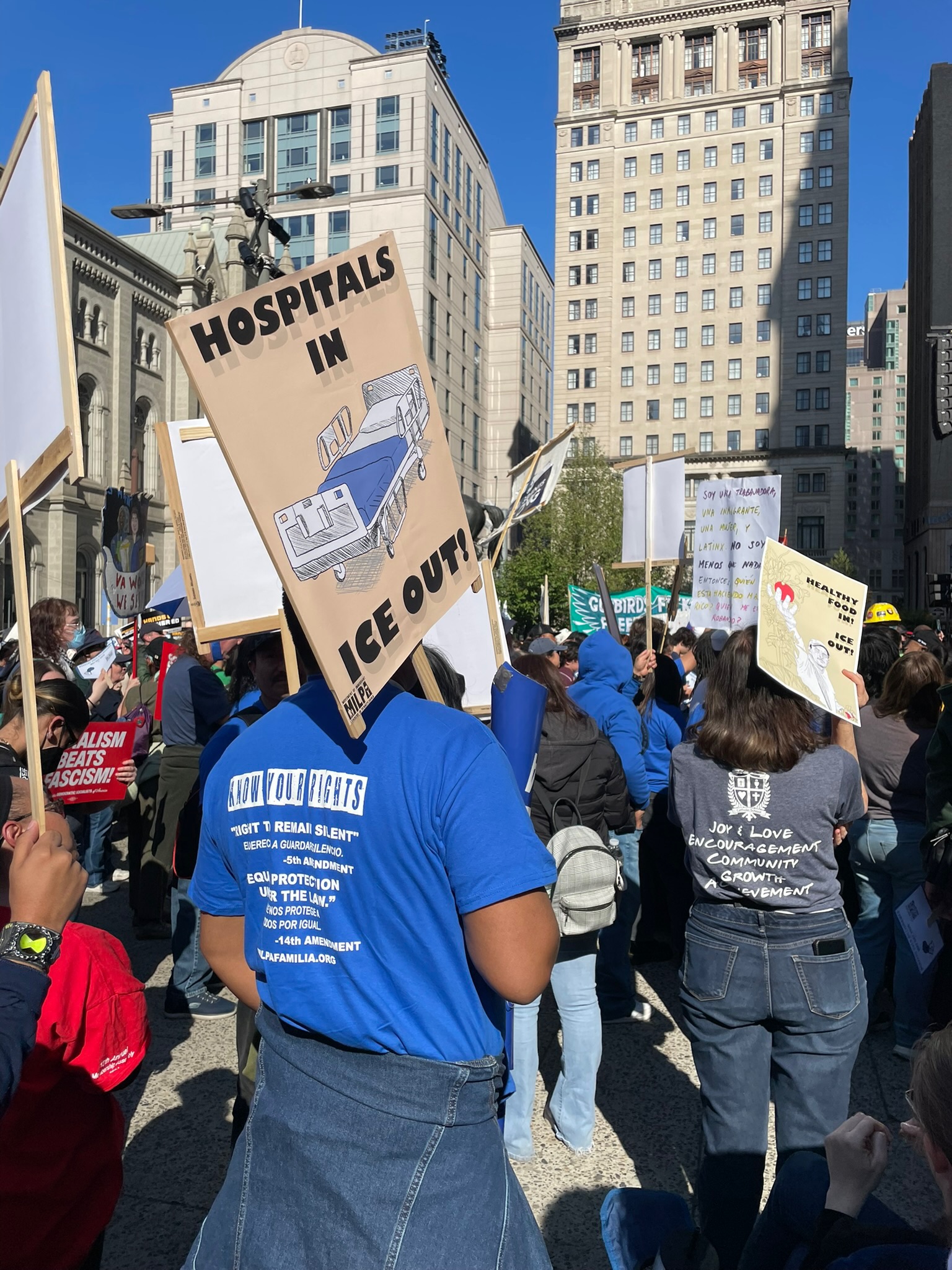
On May 1, 2026, also known as May Day or International Workers’ Day, the AFL-CIO Philadelphia lead a Workers Over Billionaires Rally and March in Center City Philadelphia. This rally was the culmination of months of unions and community organizations of our class like Put People First! PA and our sister organization, MILPA (Movement of Immigrant Leaders in PA) having thousands of conversations with our members, neighbors, families and friends to create a vision of what we need in a city that puts profit over people.
On May Day, Put People First! PA (PPF-PA) members from the Southeast PA (SEPA) region joined in solidarity for the ratifying of the Working People’s Vision for Philadelphia which was read aloud by participants from different fronts of struggle throughout SEPA, including our own leader Jeannette! Another member, Zevi, had the opportunity to hold the main banner for the parade which marched from Philadelphia City Hall to the Comcast building, where marchers called out Comcast and CEO billionaire Brian Roberts. To learn more about the Workers Over Billionaires platform click here.
Thousands flooded the streets that day uniting across lines of division. We came together across immigrants and citizens, documentation status and language, across race and religion, employed and unemployed. All for our struggle for a broad vision of living in a world where everyone’s needs are met.
Members from Put People First! PA held our “Healthcare is a Human Right!” banner because one of the ratifying points was just that: a focus on our hospitals closing, our need for preventative and emergency services, care for the whole body, including mental health, dental, maternity and more, with the demand that healthcare must be for the good of the working class, not for profit. We need our access to healthcare and we must organize to make it happen!
Do you want to join the fight for access to healthcare? Do you also believe that healthcare is a human right? Come check us out at our Facebook, website and upcoming events.
Doctoring as a Revolutionary Act by Taka Yamaguchi, Massachusetts Nonviolent Medicaid Army
“I need you to survive” I need, you to survive (A) I need you, to survive (B)
The question is not how to doctor in an anti-capitalist way (A). The question is how to make doctoring revolutionary (B).
Being a care worker and especially a doctor in our society is commodified and transactional. Commodified= interchangeable measured units to be traded and therefore profited off of Transactional= services rendered and services received, time-bounded
“A” is a technical question about how to decouple healthcare delivery from the capitalist mode of production. I’ve thought about this question for years, considering different models of healthcare delivery such as not taking insurance and using sliding scale payment supplemented with grants, etc. But it does not get at the transactional relations between “doctor” and “patient” which are baked into our society and therefore requires a larger framework to change.
“B” is a relational question. It asks, how can healthcare delivery go beyond changing the cash flow, and use the practice of “doctoring” to subvert the inhuman relationship that underlies capitalism, and to model a more human relationship for society.
Inhumanity in our society takes many forms. The obvious ones are the inhumanity that makes us look away from suffering, the inhumanity that reassures ourselves that it cannot happen to us–that it is a “them” problem, the inhumanity that makes us numb to others’ suffering in order to protect our psyches against the relentless suffering. Inhumanity also underlies liberal approaches to the alleviation of suffering. This form of inhumanity is based in pity, perhaps a sense of charity, and even a sense of goodness or ethical obligation. These ethics are still inhuman because they create a separation between the haves and have-nots. To look upon a fellow human like this is to not consider them as part of yourself, as part of a whole that includes you.
In this way even the most “social justice” oriented doctor is often acting in an inhuman way. It makes the doctor exceptional and from there the doctoring itself becomes not just an identity, but an end goal in of itself. A skill to be sharpened, a task to be performed. But I think a human (humanist?) doctor would be using their experience and skills as a conduit to become more human, to act out a mutual flourishing of our most human selves, stifled in this inhuman society.
Can a revolutionary form of doctoring make two people mutually interdependent? I think so.
The first time I saw this in action was in Palestine. I witnessed Palestinian doctors taking care of their fellow people not out of self-interest, not out of self-righteousness, but out of love. A different kind of love than that for a dear friend, or a lover, or family, but an urgent, righteous love. In genocide, the stakes are higher. Every life saved is an act of collective resistance. In every interaction, both healer and healed are reaffirmed as human while the entire world attempts to dehumanize them. Without the healed, the healer has no purpose. They might as well not exist.
A truly human community must share an unshakable faith: every single person not only matters, but is essential to collective survival, is essential to personal survival. The person in front of me must survive in order for me to survive. The act of survival is an act of reciprocity. I need you to survive. You need me to survive.
Consider the healer of pre-capitalist communities–such a role existed in all societies; depending on the geography it may exist now, or it may have been crushed millenia ago. The healer did not share their experience and skills because they expected to receive immediate returns, by and large. Neither did they give care because they wore an outfit that identified them as a healer and thus fulfilled their expected social role–this I believe is true of many doctors today. The healer healed because if they did not heal the farmer, they would starve. If they did not heal the builder, they would have no roof over their heads. In turn, if the farmer did not feed the healer, they would die of an infected snakebite. If the builder did not build for the healer, the builder’s broken arm would reharden misaligned, leaving them unable to build.
They understood that each others’ survival was dependent on everyone in the community being able to participate fully. This is a human relationship founded in love, not based on ethical ideals that it’s the “right thing to do,” but because to do otherwise was to perish alone. We know this to be true, because those who would not follow these social norms of reciprocity were cast out.
In modern capitalist society, individual survival is decoupled from collective survival. Now we praise the most inhuman and cast out those who fight to stay connected to their humanity.
We’ve used technology–physical, social, and economic technologies–to carve out physical survival in a radically different way than at any point in the preceding 500,000 years of human history. We fill our bellies with food, build shelter from the elements, even procure lifesaving medication, while our souls starve. We train ourselves to be something other than human, pretending we’re satisfied with this simulation of a fully human life. We are considered no different than machines, AI that requires carefully titrated inputs of water and food. We denigrate our innate human desire to depend and be depended upon as weakness, when in fact it is strength, a safety net that is not dependent on the whims of the rich.
Increasing numbers of us struggle to survive our death-dealing system, dealt through hypothermia in the streets, bombs on our heads, by drowning in impossible debt, or by our own shaking hands. The only way out is to organize ourselves, the poor and dispossessed, to build a united front of humanity, of human-ness. That includes those of us who are eking out a life that may be occasionally materially comfortable, but seems to leave us always wanting more, never satisfied. We ask ourselves, “is this it? Is this all that life has to offer? Some fancy toys, a few loved ones, and an unshakable sense that being alive should feel less like a battle, a chore?”
Our ruling class system has taught us that this inhuman state of existence is normal. But this past weekend at the Put People First! PA assembly reaffirmed my belief that inhumanity is not only violent and unnatural, but that we can re-learn to be human with each other. Among my roles, I was on the Health and Safety base group. In the days before the assembly, each of us in the base group were assigned to twelve “buddies” to check in on, confirm they received their COVID tests. During the assembly, we continued to check in on our buddy. All of this was done so that everyone could participate as safely and fully as possible.This was not to make sure they got their money’s worth or because we wanted to ensure a full room for the cameras. It is because every single person in the room has a story to share, everyone has a role to play, everyone is essential to making the assembly a success. Everyone depends on everyone else. If we are going to build a united movement of the poor and dispossessed, we need every single person to be fully present. It is a strategic necessity, practiced in real-time at the assembly.
A series of interactions drove this point home for me, and shook my perspective around “doctoring” to its core. A fellow leader, who had injured his knee a few weeks ago, was suffering from a flare of knee swelling as a result of an unexpectedly long car ride to the assembly. As one of the medical consults for the Health and Safety base group, I was asked to go check in on him in his hotel room. This was ten minutes before the panel on hospital closures was set to start, for which I was nervously awaiting to speak on. So I followed his worried partner to his room, and I was slightly annoyed and significantly anxious. I asked him to lay in bed, I examined his knee and asked him a few questions to reassure that he did not have any worrying symptoms of an urgent complication. I advised him to elevate his seat with cushions so he would not have to bend his knee in order to prop it up, to try gently massaging his knee with a warm towel, and told him that I would request a first-floor room so that getting up and down stairs to the main ballroom would not be a barrier to his participation.
I half-jogged, half-ran back to the ballroom so that I would be on time for the start of the panel, out of breath and brain spinning. I was introduced, not by my unadorned first name, but as Dr. Taka Yamaguchi, which made me uncomfortable because I’ve always associated that title with being exceptional, rather than a neutral descriptor for a certain set of experiences and skills. I started speaking about how the closure of children’s hospitals was disastrous to pediatric care. During my tirade against the inhuman healthcare system, I spotted my very recent patient, my fellow leader with knee pain, listening in the back with some ergonomic adjustments. At that moment, something clicked in my head. My doubt melted away.
I was overcome with love for my friend with knee pain. Or perhaps not quite love, since I had literally known him for twenty minutes, but connection, interdependence. I was so happy to see that he had made it to the ballroom, to participate, to learn and to share his learning with the others at his table or his community back home. I realized I was up there in his hotel room minutes before not because that was my assigned task, or because I happen to have this set of skills and education, but because I felt that his participation, just like everyone else’s participation, was essential to building the movement.
Our capitalist, inhuman society teaches us that some people matter more than others. It is a revolutionary idea to assert that we need all of us, that no one is less important than anyone else. And neither is this hollow idealism, some dressed up egalitarianism. This is based on a realistic assessment of what we’re up against, and it is deadly serious. In our movement to abolish poverty, we need everyone because only with everyone can we win, can we fight back against the inhuman ruling class. To leave some behind is to leave behind the most powerful weapon we have, of interdependence, of solidarity, of humanity. Does that mean that we need 8 billion people in a room before we can wrest power from the 100,000 people currently who own the world? No.
We need to practice reclaiming our humanity, to connect deeply with more and more people, so that we can get better and better at it. The forging of interdependence, of building our own safety net, is a means to an end. The revolution we seek is one to take back our humanity which has been stripped from us, to relate to each other as we used to. The ruling class does not expect us to use what they view as a weakness–stopping to lift everyone up instead of climbing over each other–against them.
At the assembly, I started to understand how caring for someone, in my case doctoring, could reflect that revolutionary value. I am doctoring because I depend on your presence, your survival, so we can all win the world we want. I am doctoring because the act is essential to me, because you are essential to me. You are part of my humanity, and I am part of yours. Only by internalizing that unity can we win against the disunity that threatens the very thing that makes us human. Without you, we will lose. I need you to survive.
*******
Taka Yamaguchi (he/him) is a member of the Massachusetts NVMA. He is a practicing pediatrician at Boston’s largest safety net hospital, and dreams of a national healthcare system that is accountable to human beings, not its shareholders. [Photo left to right: Jacob, Zevi, Taka]
What’s going on with the Crozer Health System?! Status Report: One year without Hospitals
In 2016, Prospect Medical Holdings, a for-profit private equity firm, purchased Crozer Health, the main healthcare system in Delaware County. Immediately, Prospect began looting the hospital system, making the situation worse and worse for workers and patients. They closed Springfield Hospital in 2020, followed by Delaware County Memorial Hospital in 2022 and at the same time shuttered essential services at Taylor and Crozer-Chester. Then Prospect filed bankruptcy in January 2025. On May 2, 2025, Prospect shut down the two remaining hospitals, Taylor and Crozer-Chester. Wall Street investors stole hundreds of millions of dollars from our communities, shut down our hospitals and walked away with no penalties and no concerns whether community members lived or died.
Impact:
Care for over half a million residents’ was thrown into chaos
Lost our busiest Emergency Department, behavioral health intake center and only inpatient services in the county, the only trauma center, renowned burn unit and other speciality services
Delaware County is now a maternal and infant health care desert
Riddle Hospital is beyond capacity with long wait times and is overwhelmed by patient needs
In the past year, all Crozer hospitals were sold at fire sale prices for pennies on the dollar. One hospital was sold for non-healthcare use. The other three were sold to private, for-profit groups. None of these private groups have any experience running hospitals.
Delaware County Memorial Hospital:Sold for $600,000
Sold to Upper Darby School District. Upper Darby, 6th most populated municipality in PA, remains without any prospect of a hospital opening.
Taylor Hospital: sold for $1 million & Springfield Hospital: sold for $1 million
Chariot Equities is a healthcare real estate development firm. Allaire specializes in nursing homes and rehabilitation centers, with a reputation for “turning around troubled long-term care facilities in other states”. However the company notably has several facilities in PA, NJ, and VT with high turnover rates, and serious complaints about systemic neglect and abuse in Vermont facilities. While Crozer-Chester had the county’s busiest Emergency Room and provided the many crucial services for the county, the new owners have made vague references to finding a “right-sized redevelopment strategy” raising serious concerns that only a fraction of the previous care may return. In January 2026, news broke about the shuttered Crozer-Chester Emergency Department being used for police dog training.
So what now? In the past 5 years, 26 hospitals in Pennsylvania have closed. We see mergers and closures by both for-profit and non-profit owners alike. This leaves residents without access to ongoing care. Others have cut back essential services, resulting in psychiatric, emergency and maternity care deserts.
In place of long standing community institutions, microhospitals are being built with 10-15 inpatient beds, specialty care that is more profitable for the owner, and minimal inpatient treatment options. Microhospitals are being marketed on a state and local level as the answer to unsustainable healthcare costs, but they limit comprehensive healthcare while shifting services to outpatient. As community services have been defunded over the past few decades, there are limited resources available to people.
Although the industry and policy makers use workforce shortages as another reason hospitals are closing, the underfunding and closure of nursing schools is often unmentioned. For other staff at hospitals, including social workers, nursing assistants and therapists, base pay is also often inadequate.
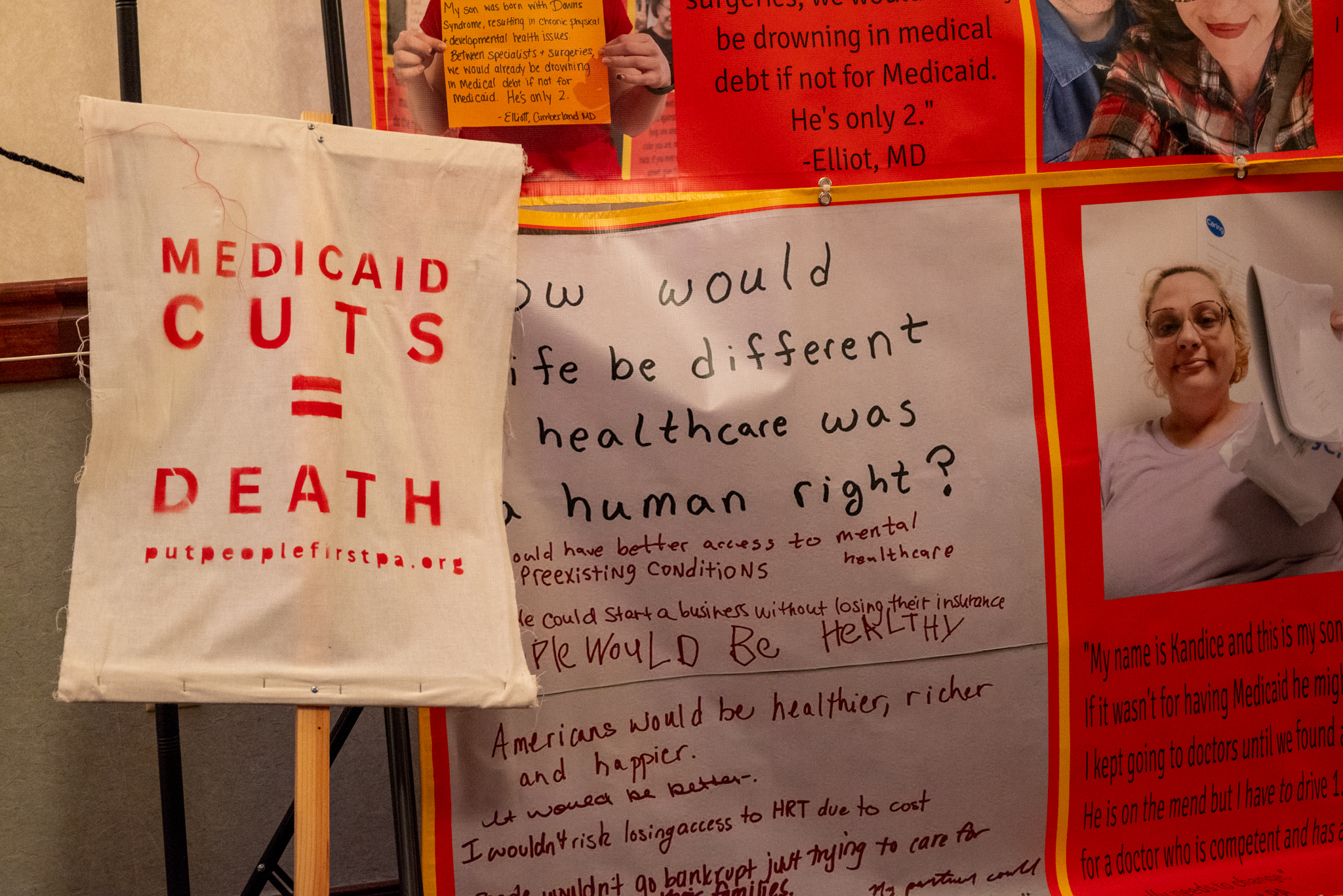
As Delaware County nears the disastrous one year mark without our hospitals, Put People First! PA is asking what do YOU need in your local hospital?
Raise your voice. Join Put People First! PA to fight back for our human right to healthcare. Click here to learn more about the actions Put People First! PA has taken to demand our hospitals reopen as community-run public hospitals. Join us as we lift up our stories and Put People First!